
Dr. Jeffrey Weitzel
Chief of the Division of Clinical Cancer Genetics and Professor, Director, Cancer Screening & Prevention Program Network, City of Hope
Follow this author
In part two of his interview with Glenn Llopis of Center for Hispanic Leadership, Dr. Jeffrey Weitzel reveals some of the work he and his team are doing to break down the previously-discussed barriers to preventative care in the Hispanic community – especially amongst Latinas who may have a genetic predisposition to breast cancer –and the many advances happening in the field of risk assessment and culturally-competent counseling and intervention.
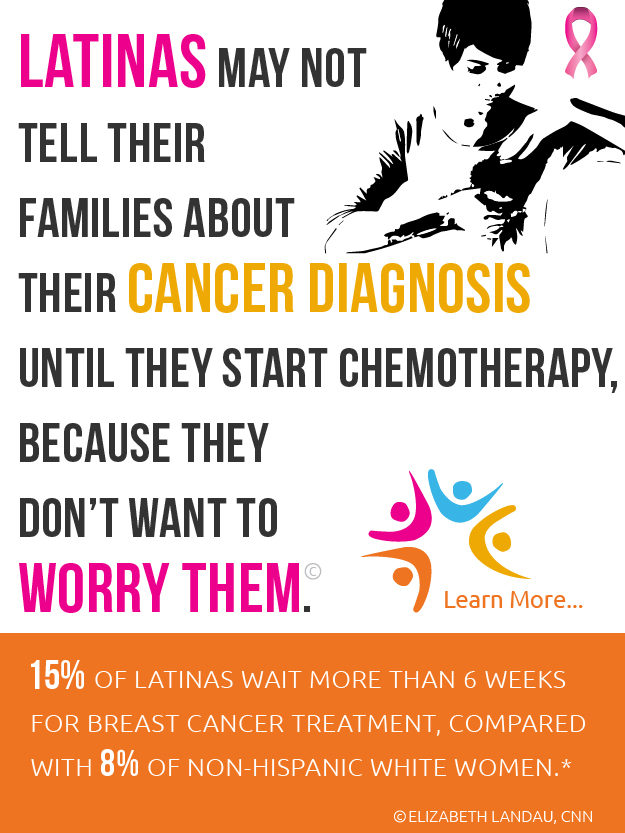
Glenn: Now that we’ve discussed the barriers keeping Latinas from getting adequate preventative care, how are you breaking down those barriers and getting the message out – especially amongst Latinas that might have the BRCA gene mutation and a higher risk of breast and ovarian cancer – without scaring them further?
Dr. Weitzel: First of all, let’s be clear that Hispanics overall have a somewhat lower risk of breast cancer compared to their Caucasian and western European counterparts. But the breast cancer that does occur in the population is typically younger age in onset, and there is an increased prevalence of breast cancer in one group of Hispanic women, those of Mexican descent.
As an identifiable subset within the population that clearly has a higher risk, these women should have access to genetic risk assessment. Getting the message out to them requires a plausible plan of action – one that emphasizes that there are kinder and gentler preventative actions you can take now that can help you potentially avoid more drastic treatment options and surgical procedures down the road.
If you present a possible path forward, instead of scaring people, you can quell the fear and override the “fatalismo” attitude that might exist – or at least change it to one of “destino,” as one colleague sees the opportunity.
Whenever I see a patient with the BRCA mutation, I make sure to tell them two things.
First, that it’s not their fault. This is an inherited mutation that goes back to Spanish Colonial times, sometimes further. You can hardly be blamed for a genetic ancestry that goes back 500 years or more.
Secondly, that what they are doing – undergoing cancer risk counseling and genetic testing – is a gift to their family. By proactively taking the first step, they’ve created an opportunity to easily and cost-effectively track the risk within their family and exercise proper screening and prevention methods to greater effect. Genetics is intrinsically a language of family and legacy, and that is a language that aligns closely with Hispanic cultural values and the desire to take care of family.
Glenn: Based on the success of your preliminary studies, has there been further research on intervention methods that would work – or not work – in underserved communities – and what would some of those methods be?
Dr. Weitzel: In other words, if we build it, will they come? If they come, will they learn? If they learn, will they do the right thing? And if they do the right thing, will they have a better outcome?
Our work covers this full spectrum, and there is evidence every step of the way that our interventions make a difference in these women’s lives based on the follow-up we do with them. But along the way, we did find that women from underserved communities were often referred to see us without adequate explanation. So they would view us as elective because they didn’t understand how seeing a geneticist was connected to their cancer treatment or why they needed to be there – and this resulted in a 50% no-show rate with the first visit, before any counseling and testing could be done.
But then something happened. A bilingual/bicultural research associate that worked with me named Veronica Lago started calling women before their first visit to collect their medical history – but at the same time she would explain WHY they were coming to see us and she also helped them prepare for the visit by getting them to collect family medical history or actual family members to bring with them.
It was a very simple intervention that made a big difference, with the first visit now reaching an 80% show rate or better. When we turned this into an actual study, we were able to show that making culturally-competent connections with people helped them to feel more comfortable coming to see us – especially when they didn’t know what to expect regarding genetics or had misgivings about it.
Glenn: How do you culturally connect with people?
Dr. Weitzel: We found that using adaptive motivational interviewing techniques (used to great psychological benefit when treating addictive behaviors) resonated on a cultural level because you’re not so much telling people why they need to come, but helping them search for their own reason for coming. You have to ask: Why do you think genetic counseling would be a good thing for you to do? What would genetic testing mean to you and your family?
By identifying with cultural values and what motivates people, by counseling people with bilingual / bicultural sensitivity, and by making them feel comfortable about being there and why, we were generating much better attendance for the initial visit, which was essential for creating bonds with the women and their families. Once they saw our commitment to them, they were more willing to commit to us, and show up for other visits.
Cultural differences aside, genetic testing has been expensive until recently, making it seem out-of-reach to underserved and underrepresented minority populations due to disproportionate economic barriers. As far as Latinas with breast cancer, we spent a lot of time learning about mutations and found that there were patterns we could exploit to provide more cost-effective testing solutions and expand access to care. In fact, we’ve even gone on the road to expand access to relatives in their native countries.
The more people we can bring in for genetic testing and counseling, the better we will understand the risk – and how we can affect that risk in meaningful ways that may also be much less intrusive the earlier that we see them.
In part three of this interview, Dr. Weitzel will talk about the ways he and his team at City of Hope are helping more people by “following the risk” – to the patient, through their families, and even back to their ancestral homelands.







Post your Comment
Please login or sign up to comment
Comments